The Levels of Evidence: How to Tell Strong Health Research From Weak
Health headlines rarely agree. One week a study says coffee protects the heart, the next week another warns it does the opposite. The confusion is not a sign that science is broken. It is a sign that not every study deserves the same trust, and researchers have a tool for sorting them: the levels of evidence.
The levels of evidence are a ranking, often drawn as a pyramid, that sorts research by how much confidence it earns. Knowing roughly where a study sits on that pyramid is the single most useful skill for reading health news without being whipsawed by it.
What the Levels of Evidence Actually Are
At the bottom of the pyramid sit expert opinion and anecdote: a single doctor’s hunch or a story about one person who tried something and felt better. These are starting points for investigation, not proof. Just above them are case reports and case series, careful descriptions of a handful of patients, useful for spotting a new pattern but far too small to establish cause.
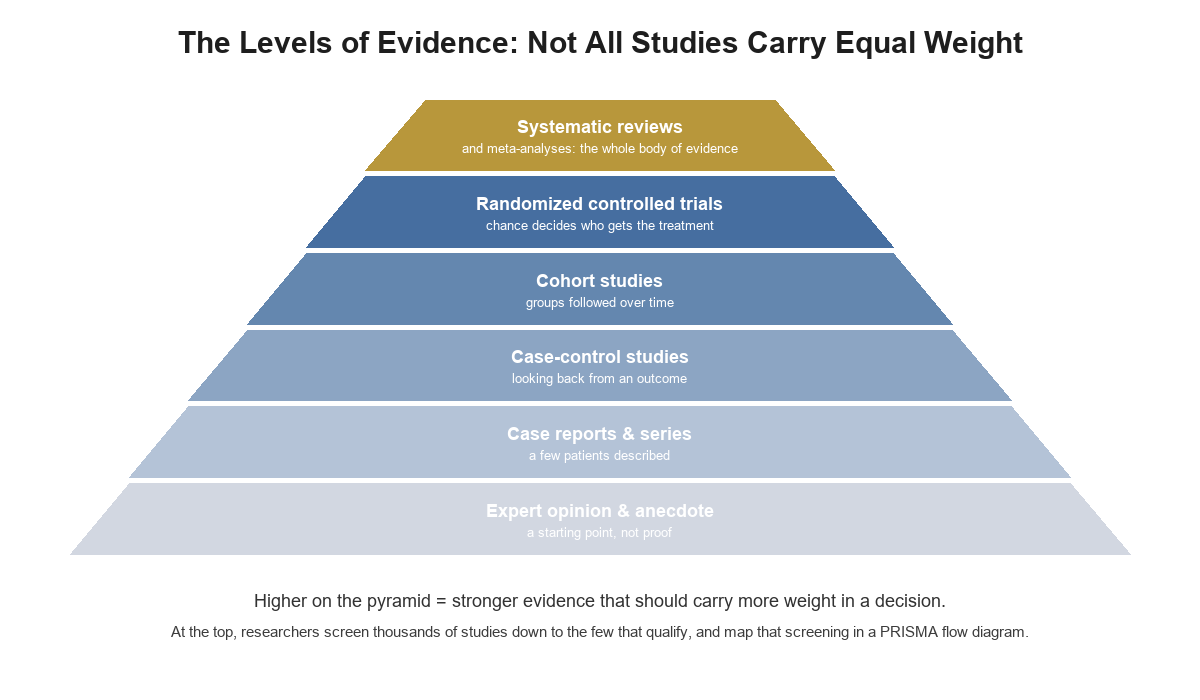
The levels of evidence, from anecdote at the base to systematic reviews at the top. Original illustration created for this article, royalty-free.
Higher up come the observational designs. Case-control studies look backward from an outcome to find what the affected group had in common. Cohort studies follow large groups forward over years. Both are valuable, but neither can prove cause, because the people being compared differ in dozens of ways at once, a problem researchers call confounding. A cohort study can show that coffee drinkers live longer without proving the coffee is why.
Near the top sits the randomized controlled trial. By using chance to decide who receives a treatment and who does not, it breaks the link between the treatment and the background differences that muddy observational research. Randomization is what lets a study claim cause rather than mere association, which is why one well-run randomized controlled trial can outweigh many observational ones.
Why One Study Is Rarely the Last Word
Even a strong single study can mislead. Small samples produce unstable results that swing from one extreme to the other. Studies that find nothing often go unpublished, a distortion known as publication bias, so the research the public sees is systematically more dramatic than the research that actually exists. And any one trial reflects one particular group of people, at one time, under one set of conditions.
This is why the practice of evidence-based medicine treats the individual study as a data point, not a verdict. The question that matters is not what the newest study found, but what the whole body of evidence says when it is gathered and weighed together.
The Top of the Pyramid: Systematic Reviews
That is the job of the two designs at the very top: the systematic review and its statistical companion, the meta-analysis. A systematic review defines a precise question, searches for every qualifying study, appraises the quality of each, and combines what they show. A meta-analysis then pools their results into a single estimate with honest error bars. Together they are the strongest answer science can currently give on a question.
The process is exacting. Reviewers often begin with thousands of database records and screen them down, step by step, to the few dozen studies that actually qualify, recording every inclusion and exclusion along the way. That screening is documented in a standard chart called a PRISMA flow diagram, which shows exactly how the pile of thousands became the handful that were analyzed. Free tools such as prismaflowdiagramgenerator.com build that diagram automatically, which is one reason the method has become the transparent standard for trustworthy reviews.
When a claim is backed by a well-conducted systematic review, it deserves real weight. When it rests on a single observational study or an expert’s opinion, it deserves curiosity and patience instead.
How to Use the Levels When You Read Health News
A few questions turn the pyramid into a practical filter. What kind of study is this, and where does it sit on the levels of evidence? Was the treatment randomly assigned, or did the researchers simply observe people who already differed? How many people were studied, and for how long? And the question that settles most arguments: what does the whole body of evidence say, not just this one headline?
None of this requires distrusting science. It requires trusting it correctly, as a slow accumulation of weighed evidence rather than a weekly stream of reversals. The next time two health headlines contradict each other, the calmest response is not to pick a side but to ask where each one sits on the pyramid, and to give the higher one the benefit of the doubt.
Read more: Why Continuous Learning Matters for Nurses Today
Read more: Mississippians’ Health Report Card Draws Attention to Gaps in Preventive Care
Read more: What High-Purity Peptides Mean for Laboratory Research




